Please stop going to the doctor for colds, flus, sinus infections, and bronchitis
A Dr. Amanda public service announcement!
One way to really do a solid for our strained primary care system is to stop going to the doctor for viral upper respiratory infections (URIs), including colds, flu, sinus infections, and bronchitis (chest cold).
You do not need our help. Stay home. Rest, drink fluids, and take over-the-counter medications for your symptoms.
Important exceptions
You’ve been sick for a while, and then you start feeling much worse
You have a sustained fever over 102 degrees Fahrenheit
You’re really short of breath or wheezing
You’re coughing up blood (not just a little speck)
You’re having severe nighttime coughing fits that make you throw up (called post-tussive emesis), and/or you know you were exposed to whooping cough
There’s anything else that’s really worrying you
(Different rules apply if you are a baby.)
A Western doctor’s job is to rule out the bad stuff that really needs antibiotic intervention, such as pneumonia, pertussis (whooping cough), or sinusitis that’s become complicated by a bacterial infection. This happens in LESS THAN 2% of sinus infections, so probably not yours :).
If you’re experiencing any of the above, by all means please call or see your health care provider as soon as you can. Everybody else, read on to learn how to diagnose and manage your own viral URI!
What to expect with a cold
You’ll probably get colds dozens of times in your life. If you don’t already know the typical symptom progression and how to recognize it, now’s the time.
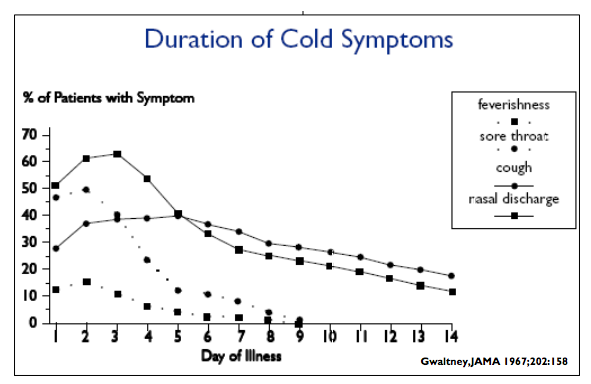
Day 1: Scratchy or sore throat, runny nose, sneezing, some fatigue.
Day 2: Mild-to-moderate nasal congestion kicks in. Low fever and more fatigue.
Day 3–4: Worsening nasal congestion. Sinus and ear pressure as the congestion backs up. Possibly a headache. Your snot might turn yellow or green, which is a normal immune response and, counter to conventional wisdom, doesn’t differentiate a bacterial infection from a viral one.
Day 5–7: Congestion improves and you’ll start to feel more like yourself, but coughing begins as your sinuses drain all of the goop they’ve produced over the last few days.
Week 2–3: Hacking, post-viral cough that usually goes away within a week or two but can linger for up to three. If you’re still coughing after eight weeks (and you’re a nonsmoker who’s not taking a blood pressure medicine called an ACE inhibitor that can cause a dry cough), then it’s finally time for you to head in to your primary care office for a chest X-ray. Something else may be up.
With influenza (“the flu”), add to the above symptoms a headache and all-over body ache that just about levels you. I’ve never had the flu, but I’ve heard it feels like death warmed over. Seriously, get a flu shot every year.
What actually helps
There are drugstore aisles full of over-the-counter (OTC) cold and flu medications, but what really works?
Interestingly, for a common cold and post-viral cough, the drugs that are together most effective at treating symptoms don’t exist as an OTC combination formula:
Pseudoephedrine, a powerful decongestant, also known by its brand name Sudafed. You have to ask the pharmacist behind the counter and show your ID to get the original pseudoephedrine because unfortunately some people use it to make meth. Don’t get the Sudafed “PE” that’s on shelves in the cold and flu aisle — it’s made with phenylephrine and doesn’t do much.
A first-generation antihistamine such as diphenhydramine (a.k.a. Benadryl), chlorpheniramine, or brompheniramine. Non-drowsy, second-generation antihistamines like fexofenadine (Allegra) are ineffective here. It’s unclear why.
A non-steroidal anti-inflammatory drug (NSAID) such as ibuprofen (Advil, Motrin) or naproxen (Aleve).
This combination is what I’ve taken to calling the secret sauce for the common cold. When you combine an antihistamine with a strong decongestant like pseudoephedrine, it’s a one-two punch that dries up your sinuses. They have totally different mechanisms of action, but both help tighten up your blood vessels to reduce inflammation. It’s this synergy that really does it. Add an NSAID with its own anti-inflammatory effect (plus pain relief), and you’ve got yourself one badass cold remedy. The evidence is pretty solid, so I don’t know why we haven’t made it a thing.
Some other good options for symptom relief are a neti pot (like NeilMed Sinus Rinse) or a steroid nasal spray (like fluticasone, a.k.a. Flonase), both of which you can get over the counter in any drugstore. All evidence aside, the important thing is to find what you think works best for you.
Here’s the closest thing we have to a cure for the common cold: sleep and hydration. Curl up, watch some Netflix, and be patient with yourself and your body.
But say you have a presentation at work tomorrow, or you’re about to hop an international flight for a snorkeling trip in the Caribbean. “Doctor, I just can’t be sick right now.” There’s now research to show that at least a couple of so-called “natural” chemicals lessen the duration of your cold symptoms in addition to their severity, most likely by supporting your immune system: pelargonium (Umcka at Whole Foods) and zinc. For them to really work, you have to start taking them in the first 24 hours of symptoms and exactly as often as directed. Zinc can give you a gross tummy ache, so make sure you always eat at least a snack before you take it. In my personal experience, the “rapid melts” are less offensively metallic than the lozenges.
For the flu, the antiviral, prescription-only Tamiflu works, but only if you start taking it within the first 48 hours. After that it doesn’t do much to alleviate symptoms or shorten the duration of the infection. Clinical guidelines recommend Tamiflu for high-risk patients (over 65, under 2, pregnant women, people with chronic illnesses, etc); otherwise we leave it up to you. And always remember your old anti-inflammatory friends, ibuprofen and naproxen, for symptom relief. (Aspirin works, too, but don’t give it to kids under 18 with a viral infection because it puts them at risk for Reye’s Syndrome.)
-----
In conclusion, save the doctor’s office for when you (and your fellow humans) really need it! Learn to diagnose and manage your own viral upper respiratory infections, and it’ll pay off year after year. Re-read this post and bookmark it for later when you feel that scratchy throat coming on…
-----
Originally published on Medium.